Category: Accidents and Incidents – Page 2
Madness on the Runway at Manchester

The Manchester Airport Group Plc owns and operates three airports: Manchester, London Stansted and East Midlands. Manchester Airport is the third busiest airport in Britain. Their website says Manchester Airport is one of only two airports with two runways. Now actually, lots of small airports have two runways (one asphalt, one grass) and the old…
Read more… 19 Jan 24
Boeing 737-900 MAX loses its cool

Well, 2024 sure has arrived with a bang. It’s a little too soon to draw firm conclusions about the MAX 9 incident, but let’s see what we’ve got so far. On the 5th of January, a Boeing 737-900 MAX registered in the US as N704AL was operating Alaska Airlines flight 1282, a scheduled passenger flight…
Read more… 12 Jan 24
A350 and Dash-8 Collision at Haneda

On the 2nd of January 2024 at 17:47 local time (08:47 GMT), an Airbus A350 collided with a de Havilland Canada DHC-8 Q300 (Dash 8) at Haneda International Airport in Tokyo. There are still many questions, but let’s put together what we know so far. Japan Airlines flight 516 departed Shin-Chitose airport, which serves the…
Read more… 5 Jan 24
Hard 737 Landing at Paro International Airport
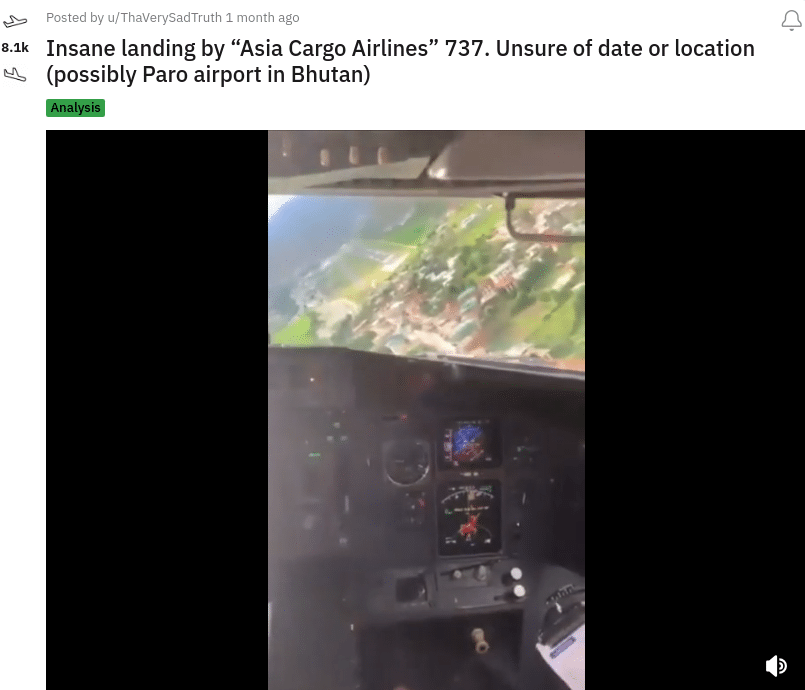
An abridged video of this landing was recently posted on Reddit. The flight took place in July 2021 and the video footage went viral in the weeks that followed. The aircraft lands safely, but it’s quite a textbook example of bad airmanship. The popular version of the video is a thirty-second excerpt where it can…
Read more… 15 Dec 23
Mid-air Collision of Wingsuit Flyer and Pilatus PC-6

On the 27th of July 2018, an experienced pilot departed with ten parachutists on board for a routine drop mission. It was the pilot’s fourth flight of the day in the Pilatus PC-6 Porter, a single-engine aircraft popular with parachuting and skydiving operations for its short take-off and landing capabilities and low maintenance requirements. The…
Read more… 8 Dec 23
Melting Windows

On the 4th of October 2023, an Airbus A321neo located in London Stansted was prepared for a multi-day charter flight in the US. There were three pilots and six cabin crew on board, as well as an engineer and a loadmaster. This first flight was repositioning the aircraft and crew from London to Orlando International…
Read more… 24 Nov 23
Accident Reports
 Air Taxi Prototype Crash at Cotswold Airport
Air Taxi Prototype Crash at Cotswold Airport
On the 9th of August 2023, a VX4 crashed at Cotswold Airport in Gloucestershire during a test flight over the runway. The VX4 is a prototype air taxi, designed and…
 The Unstallable Plane That Stalled
The Unstallable Plane That Stalled
The Cessna 185 Skywagon is a high wing, single engine aircraft: basically a Cessna 180 with six seats, a strengthened fuselage and a slightly more powerful engine. It’s a popular…
Demystifying
 Training an AI Copilot To Spot Gliders
Training an AI Copilot To Spot Gliders
My friend Maria at Daedalean wrote this article about how they are using AI to help pilots detect gliders. I thought it was fascinating and Daedalean gave me permission to…
 The Missing Bolts from Alaska Airlines flight 1282
The Missing Bolts from Alaska Airlines flight 1282
On the 5th of January 2024, Alaska Airlines flight 1282 had just taken off when it lost a door plug, leaving a gaping hole on the left side of row…
History
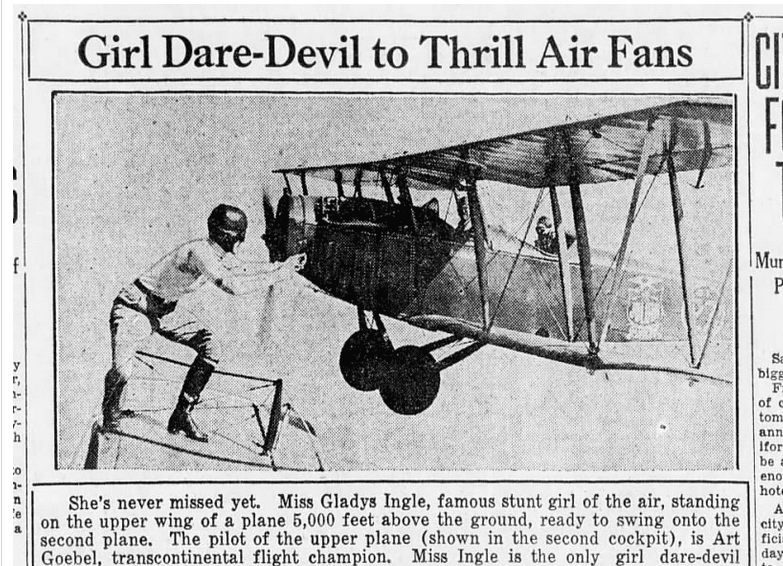 Gladys Ingle Inflight Wheel Change: Emergency Action or Stunt?
Gladys Ingle Inflight Wheel Change: Emergency Action or Stunt?
This video of a mid-air wheel exchange goes viral once a year or so, but I never get tired of watching it. Last week, it showed up on Reddit and…
 The Disappearance of the Hawaii Clipper May Not Be as Mysterious as Was Thought
The Disappearance of the Hawaii Clipper May Not Be as Mysterious as Was Thought
This week, we have a guest post by J.B. Rivard who wrote an article for the American Aviation Historical Society (AAHS) and used one of my articles as a reference.…
Fun Stuff
 A Few Good Stories
A Few Good Stories
I’m in Dresden at the moment and I’m afraid I haven’t had a free moment to write you a new article. Luckily, lots of other people are on the internet…
 Flying Fails and Airshow Considerations
Flying Fails and Airshow Considerations
Long-term readings of Fear of Landing know that my favourite aerobatics show of all time is Kyle Franklin’s Ben Whabnoski Comedy act. Just in case some of you haven’t seen…