Category: Accidents and Incidents – Page 3
The Illusion of a Perfect Landing

On the 6th of February 2010, at about half past four in the afternoon, an SAS flight took off from Copenhagen Airport for a short flight to France. Amazingly, everyone survived. The aircraft was a McDonnell Douglas MD-81. The MD-81 is the longer variant of the MD-80: a five-abreast single-aisle airliner designed as the second-generation…
Read more… 13 Oct 23
Final Report from the Contained Engine Failure of United flight 328

On the 20th of February 2021, United Airlines flight 328 made international headlines when a fan blade separated from the right engine shortly after take-off. Flight UA328 was a scheduled domestic flight from Denver International to Honolulu, Hawaii. The aircraft was a Boeing 777-200, registration N772UA, built in 1994 and powered by two Pratt &…
Read more… 29 Sep 23
Low Altitude, High Risks: Fifteen minute flight turns fatal
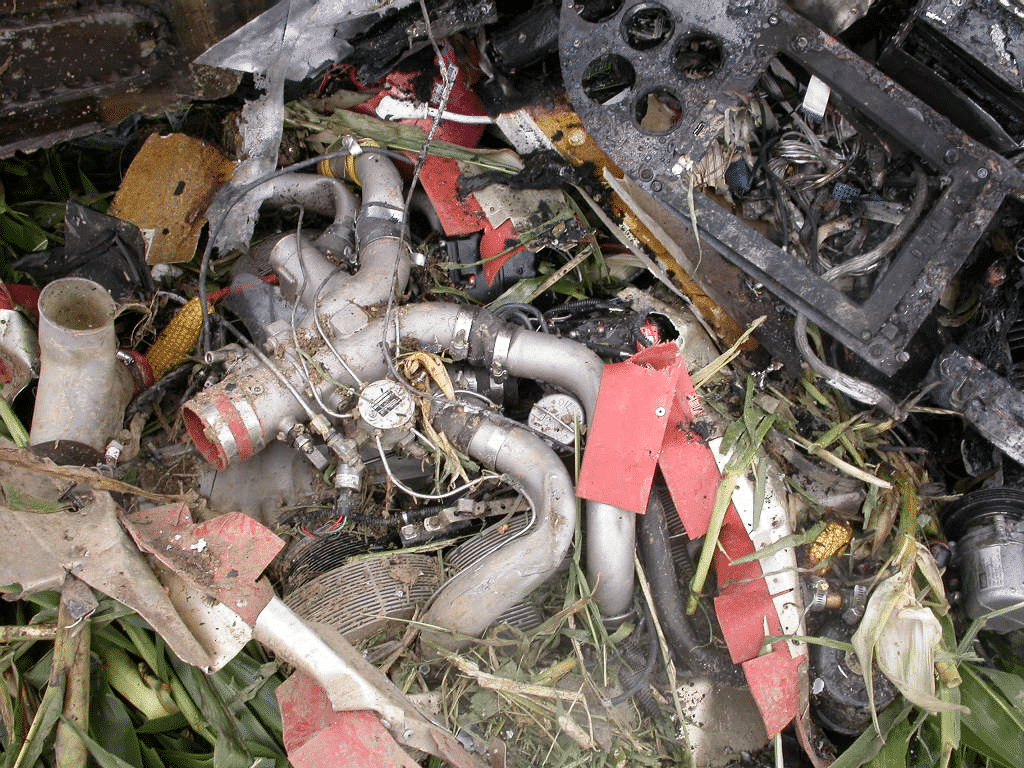
It was an overcast day on the morning of the 8th of September 2011 when people in West Liberty, Ohio, heard the sounds of a low-flying aircraft approaching. The Cirrus SR22 had left Bellefontaine, Ohio at a quarter past 11 for a short flight, just fifteen nautical miles south to Urbana, where he planned to…
Read more… 15 Sep 23
Mid-air Collision over OshKosh
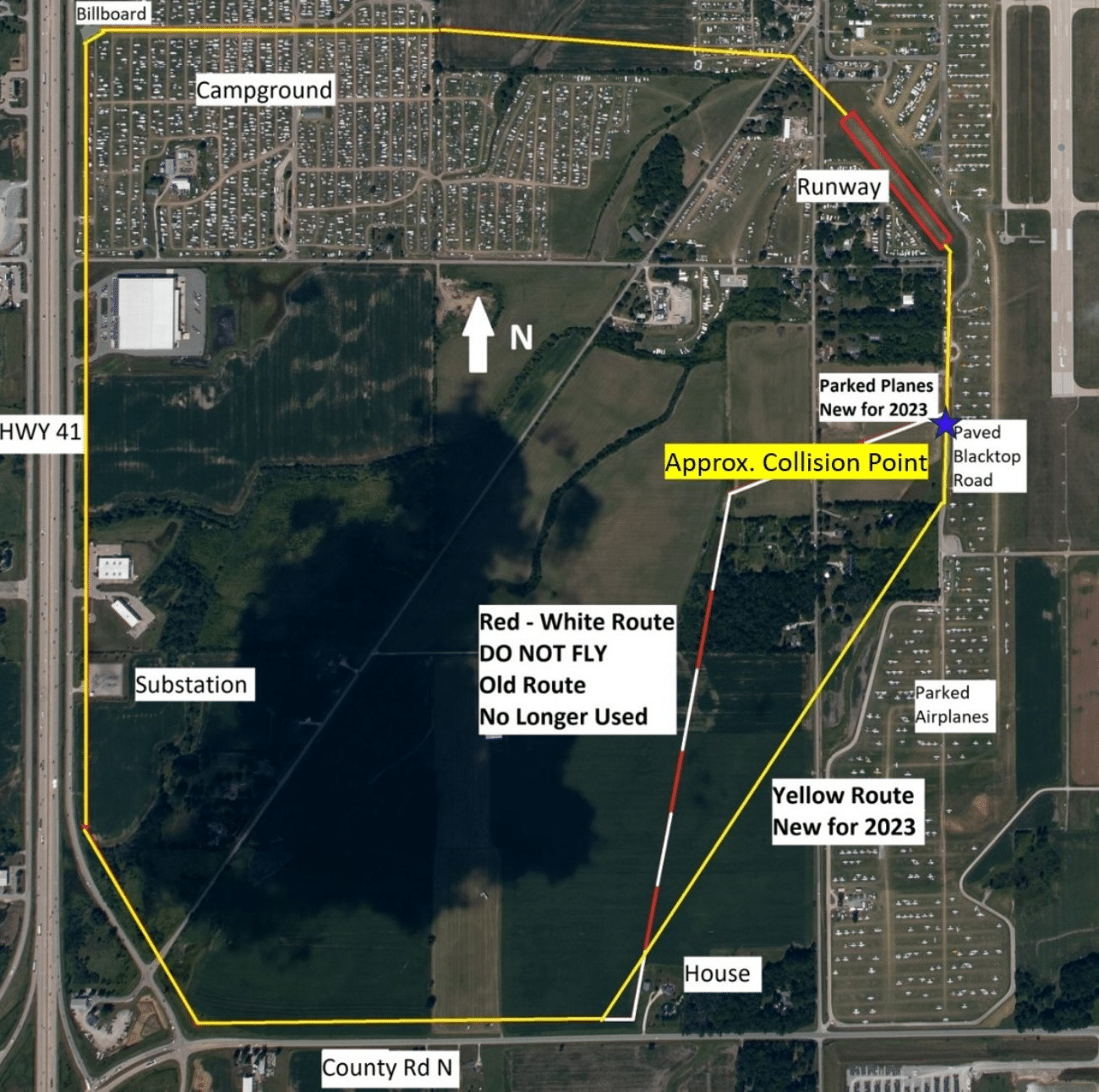
On the 29th of July 2023, a mid-air collision of a helicopter and a gyrocopter at Oshkosh left two dead and two seriously injured. The helicopter, registration N193AZ, was a RotorWay Exec 162F: a kit-built aircraft manufactured by RoterWay International. The gyrocopter, registration N221EL, was an ELA 10 Eclipse: a two-seater Spanish model. It was…
Read more… 1 Sep 23
Aircraft Collides with Lorry on Henstridge Approach
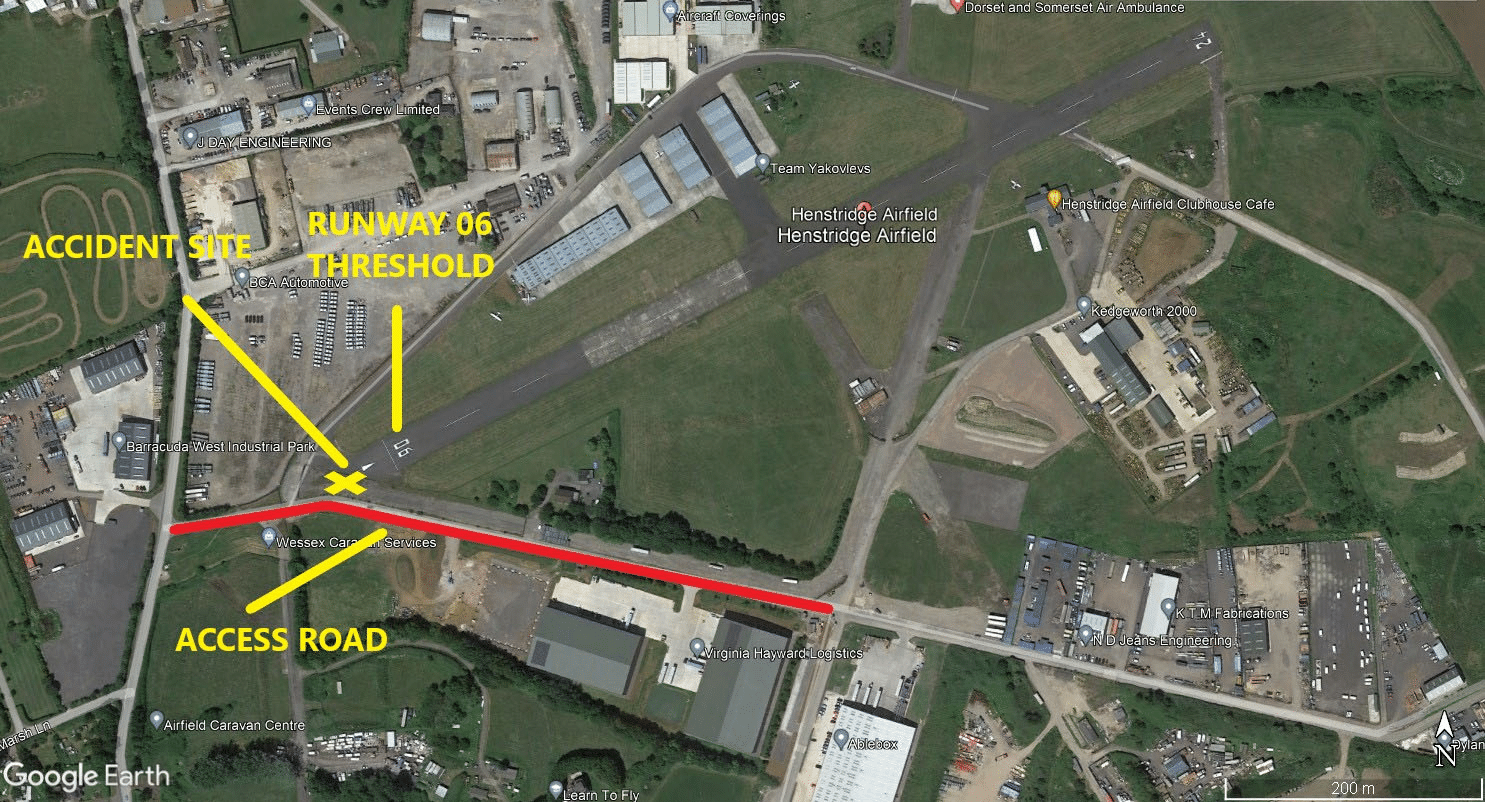
On the 2nd of March, 2023, a Vans RV-9A struck a vehicle while coming into land at Henstridge Airfield. The Vans RV-9A is a Van’s Aircraft kit plane, a kit for enthusiasts to build an aircraft themselves. The RV-9 is a two-seater low-wing aircraft; the original model is a tail dragger, but the RV-9A has…
Read more… 25 Aug 23
The “Lucky” Landing of the Tupelov Tu-154

On the 7th of September 2010, a Tupelov Tu-154M (registration RA-85684) suffered a complete loss of electrical power during a cross-country flight to Moscow. The Tupolev Tu-154 is a three-engine Soviet jet originally developed to meet Aeroflot requirements for a medium-range airliner. Production started in 1970; the last TU-154 was manufactured in 2013 by Aviakor…
Read more… 4 Aug 23
Accident Reports
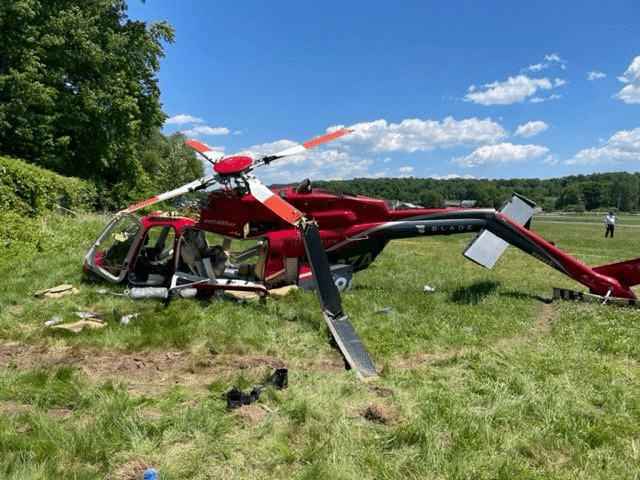 Unbolted in Fairfield (Update on the 2022 Bell 407 GXP Crash)
Unbolted in Fairfield (Update on the 2022 Bell 407 GXP Crash)
On the 4th of June 2022, a Bell 407 GXP helicopter crashed in a field near Fairfield, New Jersey. I wrote about it at the time. The final report and…
 Madness on the Runway at Manchester
Madness on the Runway at Manchester
The Manchester Airport Group Plc owns and operates three airports: Manchester, London Stansted and East Midlands. Manchester Airport is the third busiest airport in Britain. Their website says Manchester Airport…
Demystifying
 Training an AI Copilot To Spot Gliders
Training an AI Copilot To Spot Gliders
My friend Maria at Daedalean wrote this article about how they are using AI to help pilots detect gliders. I thought it was fascinating and Daedalean gave me permission to…
 The Missing Bolts from Alaska Airlines flight 1282
The Missing Bolts from Alaska Airlines flight 1282
On the 5th of January 2024, Alaska Airlines flight 1282 had just taken off when it lost a door plug, leaving a gaping hole on the left side of row…
History
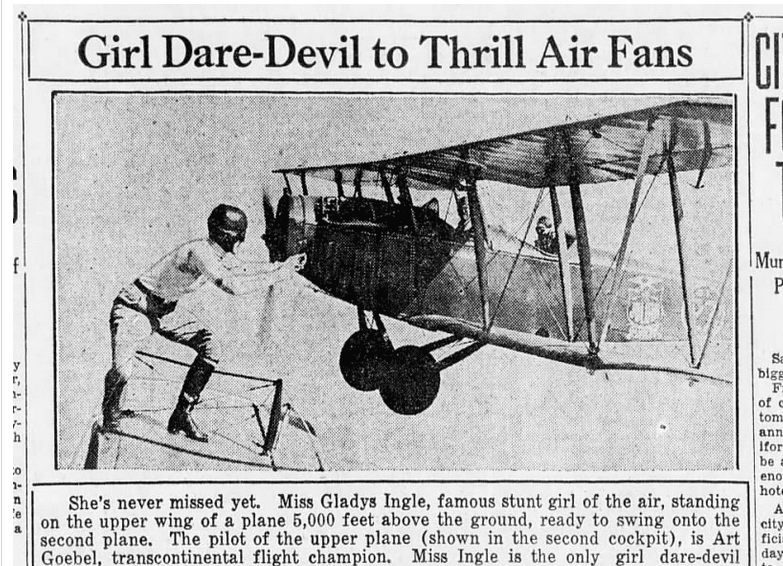 Gladys Ingle Inflight Wheel Change: Emergency Action or Stunt?
Gladys Ingle Inflight Wheel Change: Emergency Action or Stunt?
This video of a mid-air wheel exchange goes viral once a year or so, but I never get tired of watching it. Last week, it showed up on Reddit and…
 The Disappearance of the Hawaii Clipper May Not Be as Mysterious as Was Thought
The Disappearance of the Hawaii Clipper May Not Be as Mysterious as Was Thought
This week, we have a guest post by J.B. Rivard who wrote an article for the American Aviation Historical Society (AAHS) and used one of my articles as a reference.…
Fun Stuff
 A Few Good Stories
A Few Good Stories
I’m in Dresden at the moment and I’m afraid I haven’t had a free moment to write you a new article. Luckily, lots of other people are on the internet…
 Flying Fails and Airshow Considerations
Flying Fails and Airshow Considerations
Long-term readings of Fear of Landing know that my favourite aerobatics show of all time is Kyle Franklin’s Ben Whabnoski Comedy act. Just in case some of you haven’t seen…