
Latest Posts
CRJ 200 ferry flight crash with 19 on board at Kathmandu

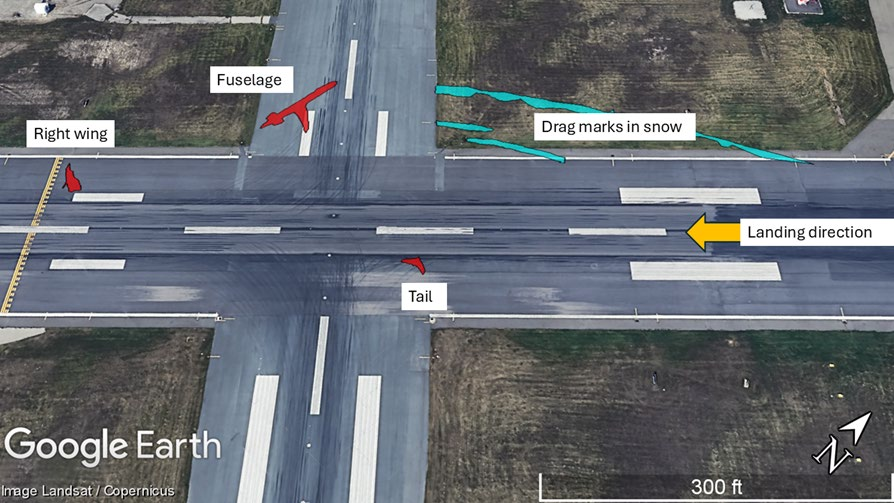
Last week, the Aircraft Accident Investigation Commission, formed by the Government of Nepal to investigate the accident of 9N-AME on the 24th of July 2024, released their final report. There’s a lot going on here, so I hope you are seated comfortably! New! You can also listen to an automatically generated audio file of the…
Read more… 25 Jul 25
Air India 171 Crash Triggered by Fuel Cutoff
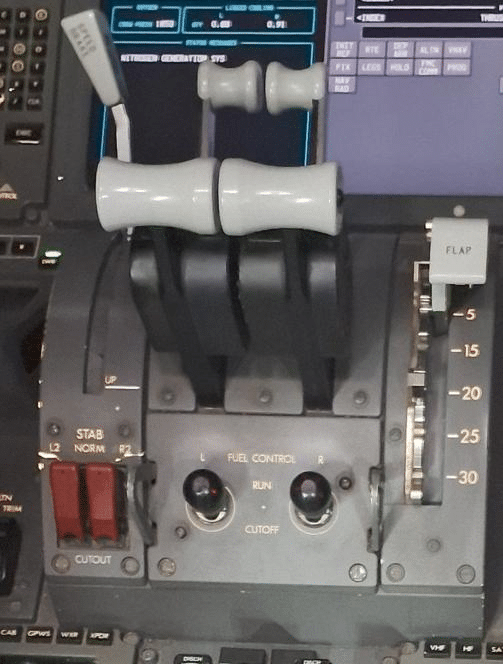
On the 12th of June 2025, a Boeing 787-8, registered in India as VT-ANB, was operating as flight Air India 171 for a passenger flight from Ahmedabad to London Gatwick. The Boeing Dreamliner crashed shortly after take off, killing all of the crew, 229 passengers and 19 people on the ground. One passenger survived with…
Read more… 18 Jul 25
How the B-52 Lands in Crosswinds

I’m here, defeated but not yet horizontal, the victim of a relentless summer cold that feels like the universe’s revenge for something I can’t even remember. If I don’t make it, please avenge me by naming a B-52 after me. I’m thinking about B-52s after watching this one land at the airshow at RAF Fairford,…
Read more… 11 Jul 25
Farewell Flight Turns Fatal in Cairns
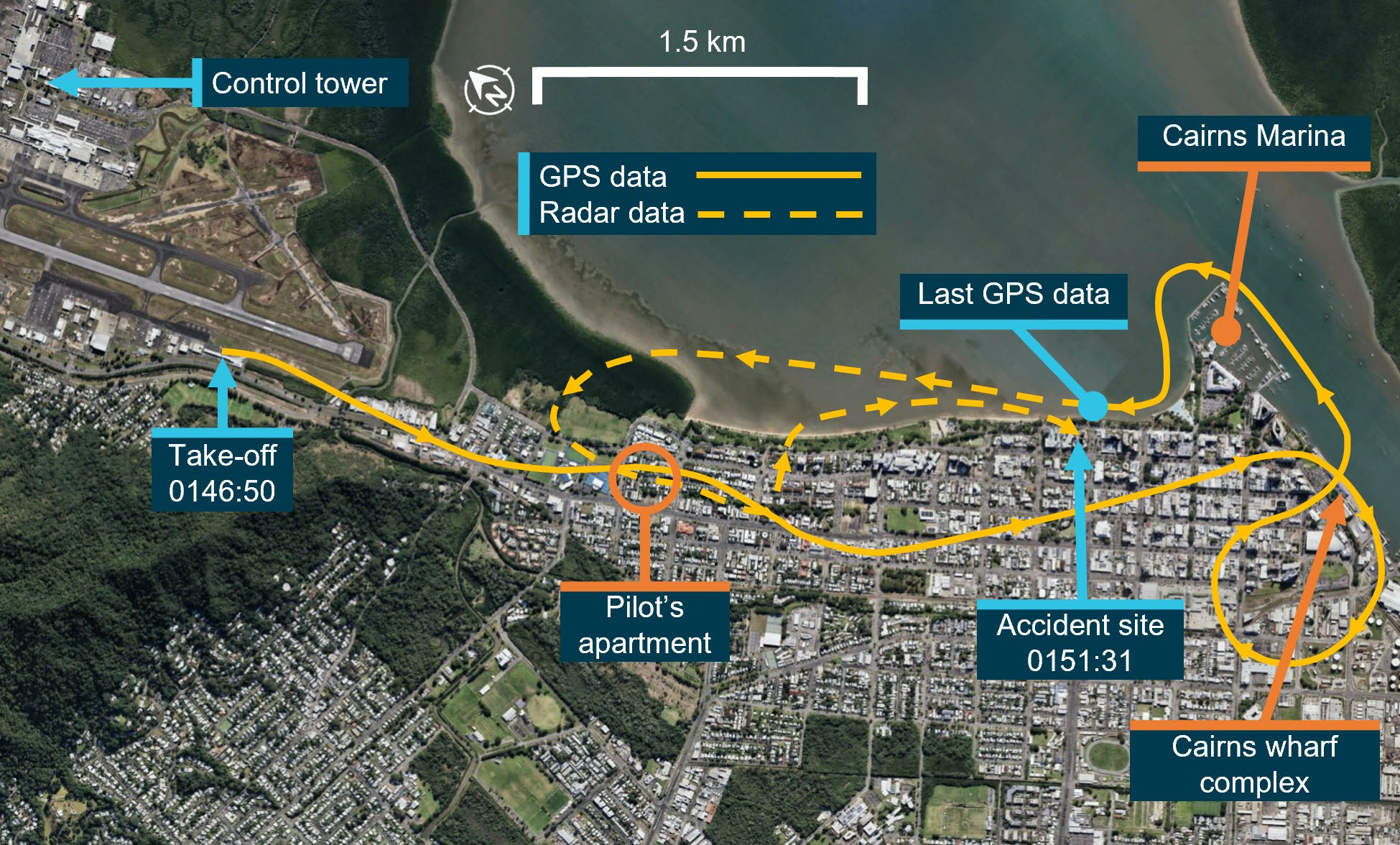
On the 12th of August in 2024, a pilot fatally crashed a Robinson R44 into the top of a hotel building in Cairns, Australia. The pilot held a commercial helicopter licence issued by the New Zealand Civil Aviation Authority, including type ratings for the Robinson R44 helicopter. He had 157.8 hours flying experience, with 16.8…
Read more… 4 Jul 25
Preliminary Reports and Key Updates on Recent Aviation Incidents
There have been some key updates on recent cases that are clearly of interest, but at the same time, they aren’t quite enough for a full-length article. Today, I’ve decided to deal with the problem with this compilation post of updates to seven different incidents, along with links to the original articles for reference. Dreamliner…
Read more… 27 Jun 25
King on a Hot Tin Roof

On Monday the 16th of June 2025, a twin-engine plane crashed onto the roof of a hangar. The aircraft was a 50-year-old Beechcraft King Air E-90, registered in the US as N1UC (serial number LW-140) with a valid airworthiness certificate until June 2031. At the time of the accident, the King Air had 10,922 total…
Read more… 20 Jun 25
Accident Reports
 No Masks, No Oxygen, No Chance
No Masks, No Oxygen, No Chance
On the 4th of June 2023, a Cessna Citation 560 aircraft crashed in Montebello, Virginia, killing the pilot and three passengers. The NTSB released their report on the 14th of…
 Hand on Thrust, Brain on Autopilot
Hand on Thrust, Brain on Autopilot
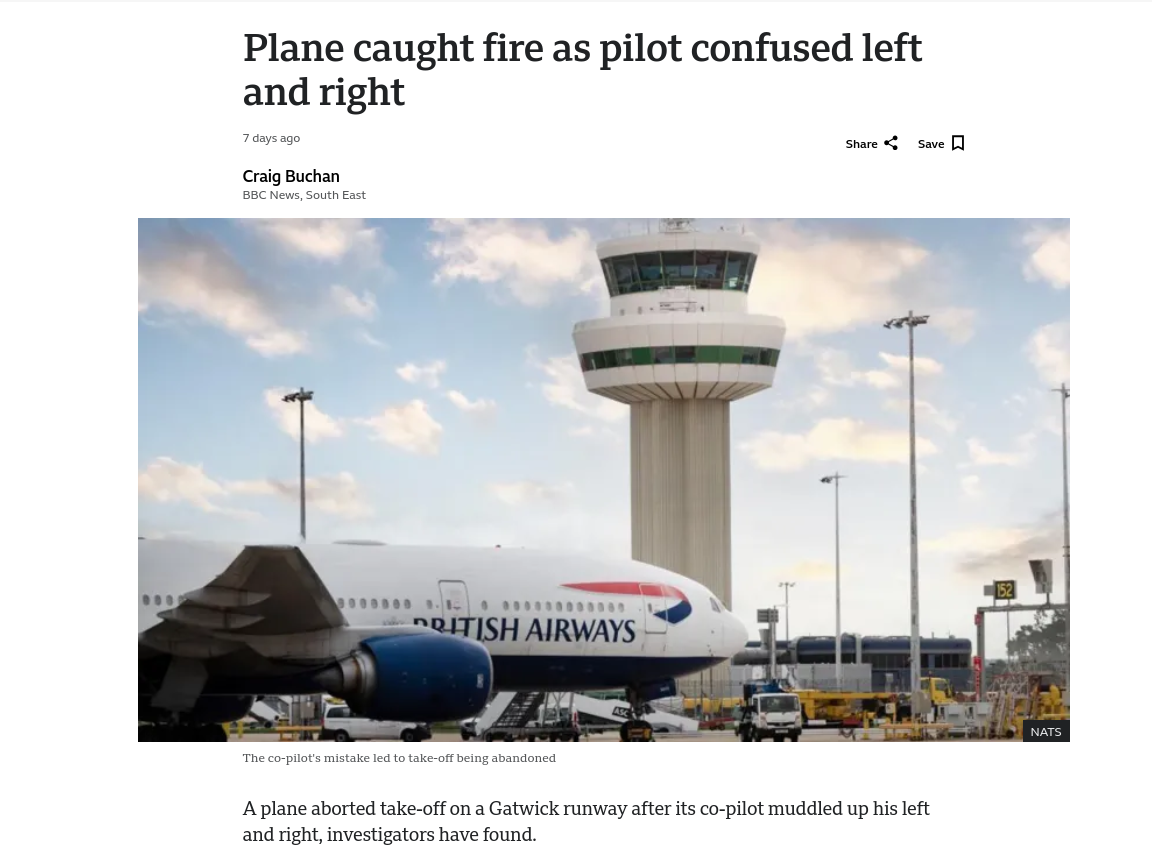
On the 28th of June 2024 a Boeing 777-236, registered in the UK as G-VIIT, rejected a take-off after reaching V1 during the take-off roll on 26L at London Gatwick…
Demystifying
 How to tell a Russian Su-27 from a British Typhoon
How to tell a Russian Su-27 from a British Typhoon
This is not an article that I ever thought I would feel compelled to write! However, given the confusion over a photograph chosen in a regional English paper, apparently it’s…
 How to tell an F-16 Fighting Falcon from a Eurofighter Typhoon
How to tell an F-16 Fighting Falcon from a Eurofighter Typhoon
There are a number of reasons why you might need to quickly point out the differences between a General Dynamics F-16 Fighting Falcon and a Eurofighter EF2000 Typhoon. You might…
History
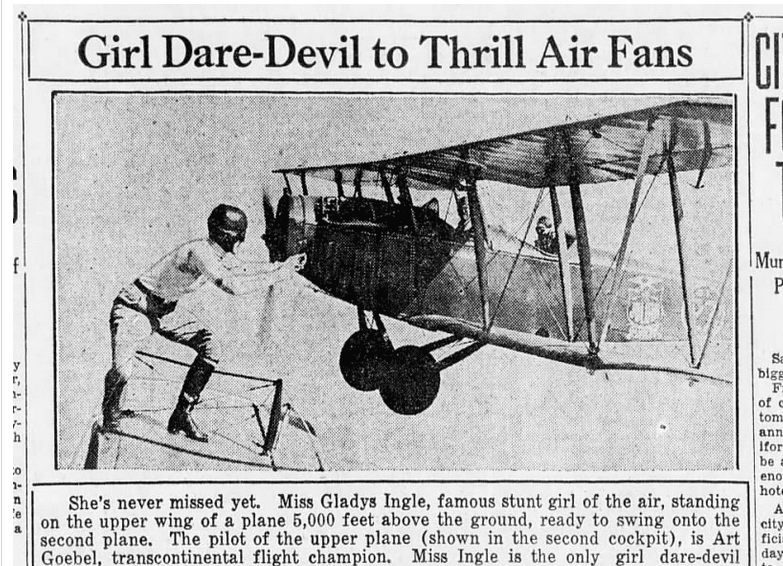 Gladys Ingle Inflight Wheel Change: Emergency Action or Stunt?
Gladys Ingle Inflight Wheel Change: Emergency Action or Stunt?
This video of a mid-air wheel exchange goes viral once a year or so, but I never get tired of watching it. Last week, it showed up on Reddit and…
 The Disappearance of the Hawaii Clipper May Not Be as Mysterious as Was Thought
The Disappearance of the Hawaii Clipper May Not Be as Mysterious as Was Thought
This week, we have a guest post by J.B. Rivard who wrote an article for the American Aviation Historical Society (AAHS) and used one of my articles as a reference.…
Fun Stuff
 Friday Lightness: A Short Respite from Crash Reports
Friday Lightness: A Short Respite from Crash Reports
It seems a good time for something a bit more lighthearted. After weeks of analyzing serious incidents and technical failures, I thought I could a moment to appreciate aviation humuor…
 Flights of Fantasy: Aviation April Fools Worth Celebrating
Flights of Fantasy: Aviation April Fools Worth Celebrating
I’m going to admit that I’m not a great fan of April Fools’ pranks, especially not attempts to trick people into believing something and then pulling the rug out from…






