
Category: Accidents and Incidents
Fatal Crash Overshadows Opening Day of EAA AirVenture Oshkosh 2024

On Monday, the 22nd of July, a Lancair Super ES crashed on approach to Wittman Regional Airport (KOSH) flying into the EAA AirVenture Oshkosh. Oshkosh is the aviation event in the US and during the event, KOSH becomes the world’s busiest control tower. For that one week, Oshkosh has the highest concentration of aircraft in…
Read more… 26 Jul 24
From Mayday to Miracle: Cessna Bellylanding at Bankstown

On the 26th of May 2024, a private pilot in a Cessna T210 Centurion II suffered an engine failure while downwind at Bankstown Airport in New South Wales, Australia. What followed was an emergency landing on video that will make you sweat. The pilot and one passenger, his wife, were on a private flight between…
Read more… 19 Jul 24
The Fenestron Factor: Cabri G2 Crash in Gruyéres

The Swiss Transportation Safety Investigation Board (STSB) has released the final report for the Cabri G2 light helicopter crash in Gruyères, Switzerland in 2022. I wrote about it at the time, but I’m repeating the information and the videos here for reference. The final report is only available in French, with no mention of it…
Read more… 28 Jun 24
Hail Damage to Austrian Airlines A320

I’ve been intrigued by the photographs being passed around of the Austrian Airlines Airbus A320 that flew into a hailstorm. We’ve seen some hail-battered planes before but this one took the nose cone right off! Austrian Airlines, a subsidiary of Lufthansa, is the flag carrier of Austria. They ordered four new Airbus A320neo aircraft in…
Read more… 21 Jun 24
Cessna 172M forced landing after go-around in New South Wales
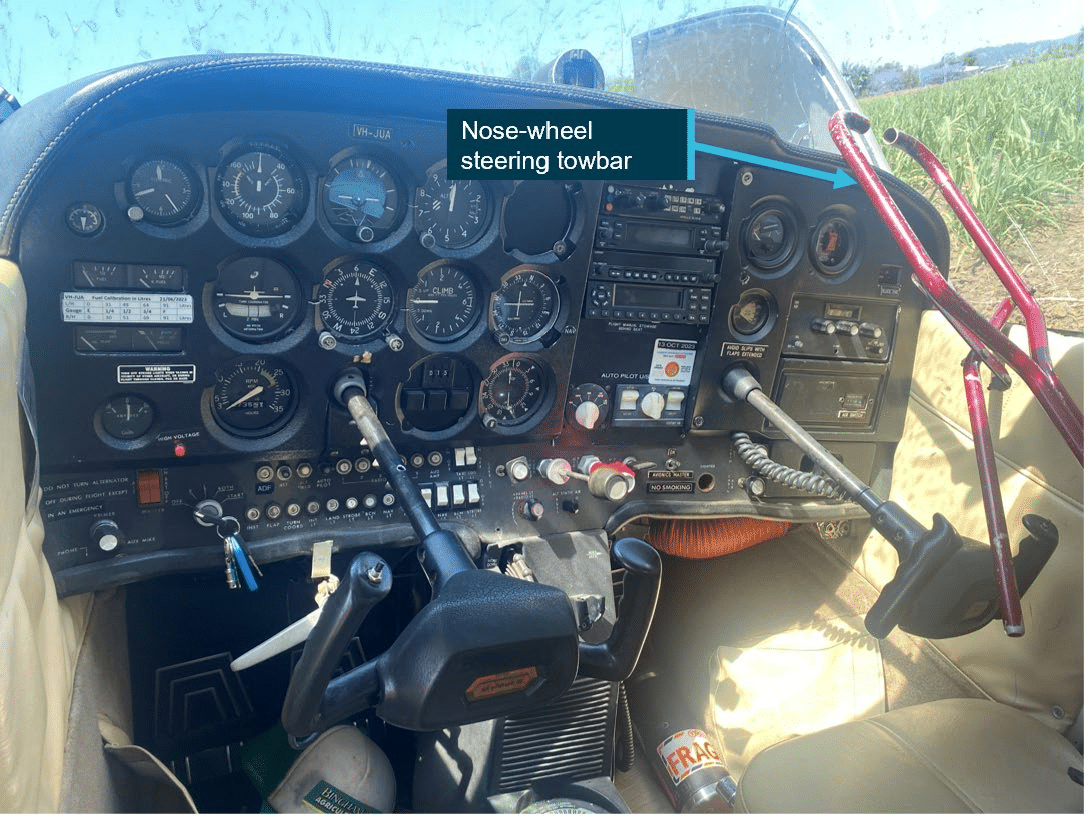
On the 15th of October 2023, a private pilot rented a Cessna 172M from Air Gold Coast for a private flight from Gold Coast Airport, Queensland, to Murwilumbah, New South Wales. The aircraft, registered as VH-JUA, was 47 years old and had been in Australia since 1989. It had over 14,000 hours, although there were…
Read more… 14 Jun 24
Continental flight 11

Sixty-two years ago, on the 22nd of May 1962, Continental Airlines flight 11 broke up at 39,000 feet. Flight 11 was the last flight of the day: a one-hour commuter flight from Chicago O’Hare, Illinois, to Kansas City, Missouri. It was a stormy Tuesday evening and only half of the seats had been sold. The…
Read more… 7 Jun 24
Accident Reports
 Air Taxi Prototype Crash at Cotswold Airport
Air Taxi Prototype Crash at Cotswold Airport
On the 9th of August 2023, a VX4 crashed at Cotswold Airport in Gloucestershire during a test flight over the runway. The VX4 is a prototype air taxi, designed and…
 The Unstallable Plane That Stalled
The Unstallable Plane That Stalled
The Cessna 185 Skywagon is a high wing, single engine aircraft: basically a Cessna 180 with six seats, a strengthened fuselage and a slightly more powerful engine. It’s a popular…
Demystifying
 How to tell an F-16 Fighting Falcon from a Eurofighter Typhoon
How to tell an F-16 Fighting Falcon from a Eurofighter Typhoon
There are a number of reasons why you might need to quickly point out the differences between a General Dynamics F-16 Fighting Falcon and a Eurofighter EF2000 Typhoon. You might…
 Extreme Turbulence in Singapore Airlines flight 321
Extreme Turbulence in Singapore Airlines flight 321
A few days ago (21st of May 2024), Singapore Airlines flight SQ321 encountered heavy turbulence on a passenger flight from London-Heathrow to Singapore. There were 229 on board, including eighteen…
History
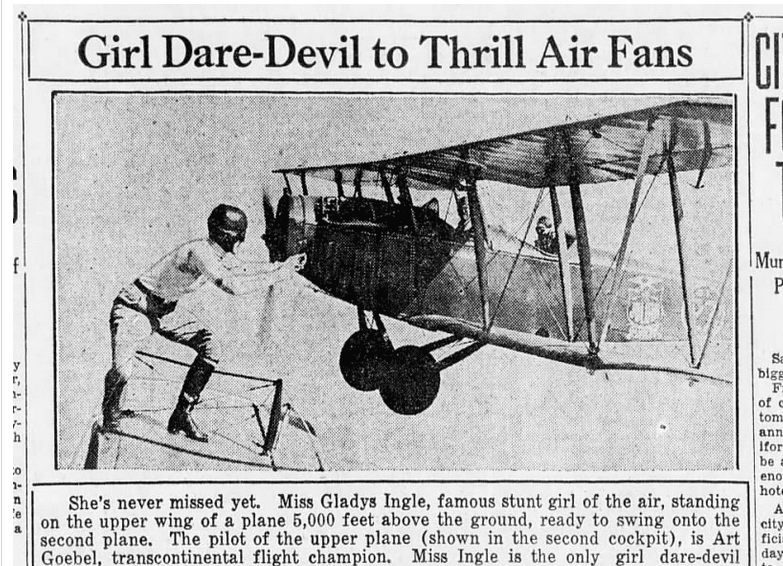 Gladys Ingle Inflight Wheel Change: Emergency Action or Stunt?
Gladys Ingle Inflight Wheel Change: Emergency Action or Stunt?
This video of a mid-air wheel exchange goes viral once a year or so, but I never get tired of watching it. Last week, it showed up on Reddit and…
 The Disappearance of the Hawaii Clipper May Not Be as Mysterious as Was Thought
The Disappearance of the Hawaii Clipper May Not Be as Mysterious as Was Thought
This week, we have a guest post by J.B. Rivard who wrote an article for the American Aviation Historical Society (AAHS) and used one of my articles as a reference.…
Fun Stuff
 Terminally Early: The Berlin Viewing Platform
Terminally Early: The Berlin Viewing Platform
Mistakes were made. All of them were mine. Before I left for Dresden, I planned out my full itinerary. Berlin is a much busier airport than Tallinn, so I needed…
 A Few Good Stories
A Few Good Stories
I’m in Dresden at the moment and I’m afraid I haven’t had a free moment to write you a new article. Luckily, lots of other people are on the internet…






