
Procedural Drift at Yeager Airport
In the early morning hours of the 5th of May 2017, Air Cargo Carriers flight 1260 crashed at Yeager Airport in Charleston, West Virginia. There were two souls on board, the two crew members, who were both killed in the crash. The NTSB took over two years to release their final report.

The aircraft was a Short SD3-30 Variant 200: a turboprop transport aircraft designed as an inexpensive and rugged aircraft capable of short-field landings. The unpressurised aircraft was designed to seat 30 passengers for short-range regional flights. Air Cargo Carriers operate throughout the US, Canada and the Caribbean; in 2017, their fleet consisted of 26 Short aircraft after the crash (twenty-five 360s and one 330), making them the primary users of Short aircraft. All of the aircraft have been converted to be used strictly for cargo. The cockpit voice recorder was removed from the 330 when it was converted for cargo use. The aircraft was in good shape and the documentation showed that it was within weight and balance limits.
The two members of the flight crew had very different levels of experience.
The captain had worked as a bush pilot in Alaska before coming to Air Cargo Carriers in 2015. He held an airline transport pilot certificate and had over 4,300 hours flight experience, with 3,700 of them as pilot-in-command.
This was the first officer’s first professional pilot job. She’d always loved flying and had previously worked as a flight attendant at another airline, where she always complained that the flights were too short. She took her ATP written exam before she even started flying, determined to make her dream come true. She was four weeks out from her check ride for CFI training when she received an offer from Air Cargo Carriers and had to make a decision whether to take the job as a cargo pilot or finish her training to look for a job as a flight instructor. She longed to fly a big airplane, said her brother, and she took the job at Air Cargo Carriers. She started her ground school and training at Air Cargo Carriers in September 2016 and built up 650 hours, with 214 total hours as pilot-in-command. Her flight time in the Short 330 were all as second-in-command.
Although she had some trouble adjusting to a schedule of night flights, she loved the new job. She told her brothers and her boyfriend how excited she was and they said that just she seemed happy to be flying. But there were some signs that her dream job wasn’t quite what she expected to be.
Her brother recalled some of her stories:
During the flight, [the captain] had pointed to something on the ground that she couldn’t see. He took control of the aircraft from her and dropped 1000 feet. He recovered it again, but the tower had asked about the altitude. She said the captain had told him it was turbulence.
She also mentioned … that there were times when he would say things like “I flew in Alaska, I got this” and she would look over and see a mountain “right there.”
Both flight crew were based at Yeager Airport in Charleston, West Virginia (CRW) and had flown together over the past six months; at Air Cargo Carriers, pilots were paired permanently rather than rostered; a captain and first officer were considered to be partners.
Air Cargo Carriers did not have a specific training course for CRM (Cockpit Resource Management); the chief pilot said it was a continuing process and reviewed throughout. Pilots are given an end of indoctrination “week 1” test which is a pass/fail exam. Failing this exam means removal from the training. They do not keep a copy of the individual results.
The director of training explained their training on CRM in an email.
I can’t say that I always use the same examples, but as we go through the PowerPoint presentation on CRM I will give personal stories about situations that have come up and how I used appropriate CRM to deal with those situations. Some stories are purely hypothetical, but I try to include as many real scenarios as possible, whether they are mine or someone has told me of a time when they used good CRM. Some stories have poor CRM practices and we discuss how things could have been handled differently and how the outcome may have changed if they were. Some stories have very good CRM and we discuss how things might have worked out differently if it weren’t for the proper use of CRM.
The chief pilot confirmed in the same email exchange that the only electronic device approved for use in the cockpit is the IPAD EFB (Electronic Flight Bag) and that this regulation was also a part of the training.
In January 2017, four months before the accident, the first officer had the following conversation with a friend via SMS.
| First officer | Just had the biggest scare of my life. Thought I was going to die. |
| Friend | Here i am dying to hear your story about almost dying |
| First officer | Okay so I got to the airport last night and there was a freakin blizzard outside. It was super windy and gusty. |
| We loaded the plane and went to take off. Once we were off the ground, we went to put the gear up and saw that the nose gear light stayed on instead of indicating that it was up and locked | |
| We cycled it a few times and nothing happened. So the captain said he’d fly while I went to look up the emergency checklist for the gear. Before I even fnished going through the checklist, we went into the clouds and lost all visual reference of the ground. | |
| And this is WV [West Virginia], there’s freakin hills everywhere. | |
| To the right of the runway is a big [expletive] hill. | |
| And we were only about 2000 ft or so above the ground. | |
| The captain wanted to get out of the clouds so he immediately turned right, where I know there’s all these hills. And he was making really really steep turns, like 60 degrees of bank and descending at like 800ft/min. | |
| And I should see [expletive] so the whole time I’m like we’re gonna hit the hills. We’re gonna hit the freakin hills. | |
| Like 2/3 into a full circle we finally broke out of the clouds | |
| And when I looked down and to my left a little, there was just a big black hole of [where] that hill was. | |
| We were super close to it. | |
| So now I’m looking around for the airport and the captain saw it and said it was behind us to the right so he started turning that way | |
| But then we went into the clouds again and it was snowing so hard and it was all white | |
| And I could tell he was kinda getting disoriented | |
| Like you know when you’re driving and the snow is coming at you in the opposite direction it’s hard to see and disorienting but now we’re also turning and descending and you have to watch your airspeed and bank | |
| And I’m watching the altimeter and I’m like okay we’re getting low | |
| When we finally broke out again, the airport was like right below us so we couldn’t line in for the runway we wanted | |
| So he called and asked to land in the opposite direction and I’m like crap, are we going to have a crazy [tailwind] on us, which is something you don’t want when you land or takeoff | |
| Luckily it wasn’t going to be a tailwind but it was going to be a [expletive] cross wind | |
| 18 knots gusting up to 30 | |
| So we went to line up for this runway and landed and when we touched down Im like thank god it’s over…but then! I think since we came in a little fast and with the crazy crosswind, it started pushing us off the runway | |
| Dude, I was for sure we were going to run off the side of the runway, up the bank and flip over | |
| The entire time the captain was like [expletive] [expletive] [expletive] | |
| lol | |
| We were only a few feet from hitting that bank on the side on the runway when he was able to turn it back | |
| Then we taxied back. The mechanic was there. We called the chief pilot and he was like yeah [just put] in the pins in (so the gears won’t retract in flight) and you should be fine. | |
| Hahha so off we went again | |
| Friend | And you made it the second time? |
| First officer | Yeah we made it. The captain was pretty shaken up though. I didn’t think he was gonna go. |
| I don’t know. I feel like we should’ve asked ATC for vectors to do an approach. We fly in the clouds all the time and when ceiling’s low, you do an approach instead of flying visual | |
| So I think we shouldn’ve done that instead of trying to get under the clouds ourselves, especially with all the hills there | |
| Yeah we had to write a report | |
| I don’t know. It’s also kinda hard for me to say since he’s the only captain I’ve ever flown with so I don’t really have anyone to compare him to | |
| But I definitely would’ve done things a little differently if I were in charge | |
| Friend | So are you gonna get a new pilot? I mean, you literally could have died |
| First officer | Nah, I’m flying with him as long as I stay in Charleston |
| Captain is sleeping. I’m gonna need you to keep me entertained for the rest of the flight | |
| Friend | Wait wait wait. There’s a pilot and a co pilot and right now the pilot is asleep and the co pilot is texting. Is that accurate? |
| First officer | Yes |
| Wait not entirely because it’s captain and first officer. I’m pilot too, you know! | |
| And I’m the one flying right now | |
| Friend | Jesus Christ |
| First officer | Texting and flying because texting and driving is played out lol |
| Friend | How are you texting? I mean signal wise |
| First officer | I guess I’m still getting signal. We’re only at 8000. |
| Sometimes I get it and sometimes I don’t. | |
| Can you imagine if this plane had autopilot? We’d both be asleep hahhaha |
The flight crew met up at Louisville International Airport at just past midnight the day before the flight. They departed at 04:50 and arrived at Charleston’s Yeager Airport at around 6:30 in the morning. The captain used a CPAP (a breathing device to combat sleep apnea) which showed to have been in use from 07:12 to 15:11. His girlfriend remembered that he got up and cooked dinner for them and started getting ready for work around 21:00. The first officer’s morning schedule isn’t known but she sent a text message around 13:30 and spoke to her brother on the phone for some time that afternoon. She cooked dinner and then spoke to her brother again before leaving to meet the captain at the airport.
They flew to Louisville, arriving just before midnight, ready for their scheduled cargo flight from Louisville back to Charleston.
It was 05:41 on the 5th of may when they departed Louisville on an instrument flight rules (IFR) flight plan and climbed to their cruising altitude of 9,000 feet. They picked up the automatic terminal information service (ATIS) information November with the 05:54 weather for Charleston: wind from 080° at 11 knots, 10 miles visibility, scattered clouds at 700 ft above ground level (agl), and a broken ceiling at 1,300 ft agl.
However, just before 06:30, the broken cloud ceiling dropped from 1,300 feet above ground level to 500 feet. The weather observer edited the special weather observation to note valley fog, a few clouds at 100 feet and an overcast layer at 500 feet. These observations are automatically sent to ATC however the tower controller, who expected the weather to change again in a short time, decided that it wasn’t worth updating the ATIS for this special observation. He finished his shift around 15 minutes later and didn’t brief the arriving tower controller that the ATIS wasn’t current. At 06:54, directly after the accident, the weather was recorded as wind from 230° at 3 knots with ten miles visibility, few clouds at 100 feet above ground level and an overcast ceiling at 500 feet above ground level.
A new ATIS recording should be made for any new official weather, whether or not there is any change in values. Air traffic controllers are expected to inform flight crew if either the ceiling or visible is below basic minima if that information was not included in the ATIS. But neither of these things happened.
The first officer contacted Charleston approach at 06:37. The controller told them to expect localiser approach to runway 5, which has a minimum descent altitude (MDA) of 1,320 feet above mean sea level or 373 feet above airport elevation, with a minimum visibility of 5,500 feet runway visual range.
The controller told them to expect localiser approach to runway 5, which has a minimum descent altitude (MDA) of 1,320 feet above mean sea level (amsl) with a minimum visibility of 5,500 feet runway visual range. The first officer, presumably on the request from the captain, asked for the VOR-A circling instrument approach instead.
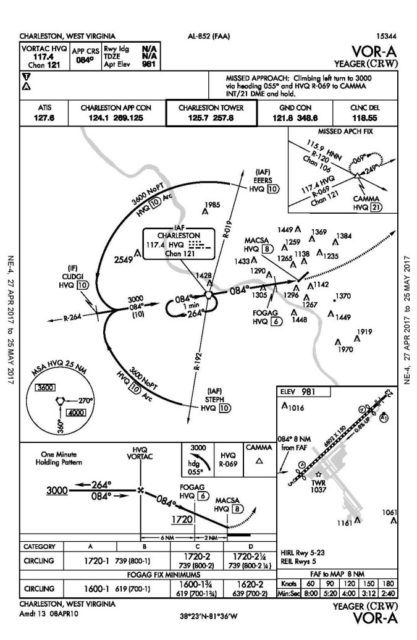
The VOR-A instrument approach is a circling approach because the final approach segment is more than 30° different from the alignment of the runway (runway 5 in this case). This approach has a minimum descent altitude (MDA) of 1,600 feet amsl and minimum visibility 1 mile upon crossing the FOGAG waypoint. At that point, the flight crew should not descend further until the runway is in sight and can be reached “at a normal descent using normal maneuvers”, where in this situation, a normal descent would be about 500 feet per minute.
If the flight crew does not have visual contact with the runway by the time that they have reached the missed approach point, then they follow the missed approach procedure which in this case is to initiate a climbing left turn to 3,000 feet above mean sea level.
At Air Cargo Carriers, the standard operating procedure was to use the localiser approach if it was available. It is a straight-in approach aligned with runway 5, which is great if you were coming from that direction. They weren’t. It seems likely that the first officer requested the VOR approach because it lined up nicely with their flight path, whereas the localiser 5 approach meant a slightly longer flight to the airfield.
When the first officer contacted the Charleston tower controller, she initially stated that the flight was on a visual approach and then corrected herself to say that it was the VOR-A approach. The tower controller now on duty agreed and cleared the flight to land. About two miles out from the FOGAG waypoint, the aircraft descended below the minimum-step-down altitude by 120 feet . An alarm sounded in the tower and the controller contacted the first officer to issue a low-altitude alert. The first officer responded to say that they were at 2,200 feet and getting down to 1,600 feet (the minimum descent altitude).
The VOR-A circling instrument approach had a minimum descent height of 773 feet above the ground, compared to the localiser 5 approach which allowed a descent to 373 feet above the ground (technically speaking, above the elevation of the runway threshold). On that night, the clouds were at 500 feet, which meant that the crew would be unlikely to make visual contact with the runway using that approach. But although the weather observer had noted the valley fog and low cloud over the airfield, the tower controller had not added it to the ATIS recording. About fifteen minutes later, his shift ended and he didn’t think to mention it to the next controller. The ATIS information still said that there was a broken cloud ceiling at 1,300 feet above ground level, which meant that the VOR-A circling instrument approach with a minimum descent of 773 feet was fine.
The tower controller replied that the alarm might have been triggered by the descent rate, which was somewhere between 1,300 and 2,000 feet per minute.
The aircraft levelled off at 1,600 feet. A witness on the ground saw the Short 330 as he was driving down a hill about two miles east of the approach end of runway 5.
From the investigation:
He stated, “it was a beautiful sight” [and] the airplane was “hugging” the bottom of the clouds, “just grazing the bottom of the cloud or fog deck.” He stated he saw the landing lights and the shadow of the airplane perfectly as it headed towards him, then it passed directly overhead. He thought the airplane was on the VOR-Alpha approach.
About half a mile from the displaced threshold of runway 5, presumably at the moment when the runway became clearly visible, the aircraft suddenly entered a steep left turn, descending at 2,500 feet per minute. The Short 330 reached a 42° bank angle as the captain attempted to line up with the runway. Then the aircraft pitched nose up. The descent rate reduced to about 600 feet per minute, likely caused by the captain pulling up hard as they raced towards the asphalt. However, it was too little, too late.
The aircraft’s left wingtip struck the runway 5 centreline with the aircraft in a 22° bank and a 5° nose-down attitude and an airspeed of 92 knots. The left-landing gear and left propeller crashed into the pavement and the left wing separated from the aircraft as it slid off the left-side of the runway and down a hill, coming to rest in the trees.
The crash was captured on CCTV (if reading in email, you may need to click through to the post to see the video):
There was no chance of survival.
When investigators arrived, they found the aircraft scattered around the runway and the rough ground.
The flight deck was damaged and distorted. Both power levers were found at the “Flight Idle” position and both fuel levers were found at the “Ground” position. The left propeller lever was found in an aft position, and the right propeller lever was full forward. The flaps handle was in the 35° detent. Both control columns were broken at the base and had partial movement in the forward/aft and left/right directions. Both control wheels were jammed in a full-right-turn position. Both rudder pedal assemblies were deformed, and the left pedals were missing. The control column bases, control wheels, and rudder pedals remained coupled and moved together.

Why had the flight crew tried such a messy last-minute manoeuvre rather than just go around? The crew did not appear to be under any time pressure and there was no reason to believe that the captain had been fatigued. However, investigators found that the captain was known to have some performance issues, including a checkride deemed ‘unsatisfactory’ based on poor instrument flying. Although the captain had thousands of hours of flight experience, the investigation found evidence that he was not comfortable with instrument flying. It seemed that he felt more confident that he could pull off an unstable approach than the approach on the localiser.
The first officer should have called for a missed approach but she was a lot less experienced than the captain and, based on interviews with her friends and family, she was hesitant about speaking up as she was new. The company had not shown any signs that they would support a less experienced pilot complaining about her captain, a captain to whom she was assigned to as a partner.
Besides, this wasn’t the first time he’d flown into Charleston like this. The flight crew had landed at Charleston seventeen times over the past month. On three separate VOR approaches, the captain had descended below the minimum descent altitude while in instrument conditions.
Also, both flight crew consistently turned late onto final and at a lower altitude than recommended by the airline’s standard operating procedures. Airport security footage videoed the base and final leg of the flights for runway 23. When the NTSB reviewed these visual approaches, they found that the final approach, whether flown by the captain or by the first officer, lasted just 12 to 39 seconds, compared to the 75 seconds for the final leg as required by Air Cargo Carrier’s standard operating procedures.
This is a clear example of procedural drift. Procedural drift is the mismatch between textbook compliance and how procedures are followed in the real world. Procedural drift in some form (descriptions vary) appears as a primary or contributing cause in the majority of aviation accidents. Simple shortcuts and willingness to take risks slowly erodes the safety nets put in place. When a pilot in a rush skips a checklist without issue, it becomes easier to skip it next time. When a second pilot accepts this as reasonable, both will soon begin to skip the checklist or in other ways become apathetic to standard operating procedures. If management does not appear to care and training appears simply to be ticking the box, procedural violations are not seen as a big deal.
In this case, a pilot with 4,300 hours was paired with a newly qualified pilot with 650 hours. Once flying together, they received little or no external input. This is an environment which makes it easy to lose sight of the importance of specific procedures. Over time, the captain started to take short cuts in order to focus on other issues that they see as more important — in this case, a stabilised approach was not seen as important as landing the aircraft quickly. The first officer initially expressed concern but over time, she too began flying into their home airport low and with a late turn to final.
These changes to established procedure continued to drift, until there was a glaring gap between the standard operating procedures and reality.
At Air Cargo Carriers, once a pilot was assigned a base and started flying, there was “no real scheduled oversight” according to the director of training. “Annual recurrent, and that was it.” It was hard, he said in interview, to know what they were doing.
However, it wasn’t that difficult to know where the captain’s weak spots were.
A review of the FAA’s complete airman file for the captain found several notices of disapproval going back to 1999. Most recently, during the ATP certificate checkride, on July 22, 2016, the captain received a notice of disapproval due to excessive deflection of both the glideslope and localizer for an instrument landing system approach, repeated glideslope and sink rate warnings from the ground proximity warning system, and his subsequent failure to initiate a go-around. He passed the practical reexamination 3 days later.
At airlines where various crew are paired together based on a roster, each crew member gets to learn from different people, particularly important in a case like the first officer’s, where she had low hours and not a lot of experience. But also, the captain might well have been corrected by another, more experienced first officer. If the first officer had flown that same unstabilised approach with another more skilled pilot, her approach would have been corrected. It could also have given her the opportunity to report the concerns that she had shared with her brothers and her friends.
By varying pilot pairings, there are multiple chances to catch procedural drift from standard operating procedures before they become ingrained.
The chief pilot at the airline was asked about the pros and cons of permanent crew pairings after the accident and conceded that a negative aspect was that people could pick up bad habits. The airline did not have any formal program for reporting or documenting safety issues or irregularities. For the first officer to highlight the issues with her captain, she would have needed to phone or e-mail either the director of training or chief pilot. Such reports were not logged or tracked; the only operational oversight was the annual recurrent training. The chief pilot said that he normally checked in with new-hire pilots after the first week on the job to see how they were doing — however, no one checked in with the first officer after she started. The chief pilot said that he assumed if pilots were having difficulties, they would reach out.
Probable Cause:
The National Transportation Safety Board determines the probable
cause(s) of this accident to be:the flight crew’s improper decision to conduct a circling approach contrary to the operator’s standard operating procedures (SOP) and the captain’s excessive descent rate and maneuvering during the approach, which led to inadvertent, uncontrolled contact with the ground.
Contributing to the accident was the operator’s lack of a formal safety and oversight program to assess hazards and compliance with SOPs and to monitor pilots with previous performance issues.

Air Cargo Carriers learnt the hard way that CRM is not just about how two pilots interact with each other in the cockpit. It is not simply a case of giving the right theoretical answer when presented with an example with an obvious conclusion. CRM starts at operations. Pilots should be paired to avoid steep authority gradients and everyone at the company needs to support a healthy safety culture. Pilots must have trust in their management and they must feel secure that they are expected to report possible safety concerns. Standard procedures need to include following up with flight crew to ensure that possible issues are highlighted early. And when such issues arise, they must be documented.
References:
- National Transportation Safety Board Aviation Accident Final Report DCA17FA109
- NTSB Operations/Human Performance Interview Summaries
- Excerpts from NTSB Email Correspondence with Air Cargo Carriers
- Air Cargo Carriers CRM PowerPoint
- Procedural Noncompliance: Why Pilots Don’t Always Play By The Book
- FlightGlobal: NTSB gives details of 2017 Shorts crash as video surfaces







Another sad story, a totally avoidable accident. Already reading about the antics of the captain it became clear that this was another sad case of an experienced bush pilot who has problems with the transition to a multi-crew IFR operation. And unfortunately the F/O never really had a chance. She never was trained properly and never really knew the difference between a proper and a (far) below standard operation. Permanent pairing of a crew is not a good idea, especially if the F/O is inexperienced and the captain is weak.
A crosswind component of 30 kts is just over the limits for an SD 3-30. The main difficulty comes not when the aircraft is still flying, not even when touching down. The Shorts was not pressurized, the cabin had a nearly square cross-section. It was also known as the “Vomit-Comet” or the “Flying Shed”. Because the cabin was slab sided – very good for loading cargo – it caught the wind side-on. Once on the ground the control yoke had to be held hard into the wind, or the aircraft could be blown over and on to its wingtip. Once the speed was under control and reduced to taxy, the gust lock was applied. Steering on the ground was by a “tiller” on the side of the cockpit. The captain had to push down (right) or pull it up to turn left. The pressure had to be held constant, the nosewheel followed the commands in its own good time. Applying more force on the tiller did not increase the response. After a while the pilot would get used to it.
From what Sylvia writes, it seems that the aircraft got too slow in a steep turn, my guess is that it stalled.
BTW: I think that the procedure as described is not a “circling”, but an “arc” approach. A circling approach is a cloud-break procedure: an instrument approach, followed by a visual circling manoeuvre for a landing on another runway. Of course, the minimum for a circling has to be higher than MDA for the approach if followed by a landing on the runway for which the approach has been drawn.
During an arc approach the crew maintains a constant distance (VOR-DME) from the facility. If the distance increases, the pilot decreases the radius and of course, if the DME shows a decreasing number the crew will turn a bit less. An RMI that can be coupled to the VOR is a near necessity. Once passing a certain radial, the crew then can turn in to capture the inbound VOR radial, or a LLZ if available. The aircraft should be at a certain “platform height” when establishing on the final track, and at a certain distance start the descent in accordance with the procedure. It requires a bit of practice but when mastered it is actually quite a nice way to fly the approach. I used it quite a few times flying an ATR 42 or Shorts 3-60 into Donegal airport, Ireland. It was drawn to assure a safe distance from the surrounding terrain. Donegal-Carrickfin did not have radar, so it was important to fly the arc properly.
I had a reaction similar to Rudy’s. Flying a fairly light aircraft in bush pilot conditions requires a great deal of stick and rudder skill, and for a pilot to be able to react quickly. These skills are good for any pilot, but in flying IFR in more complex aircraft, you can’t rely solely on seat of the pants skills. Even the transition from a fixed gear single engine aircraft to a more complex single engine aircraft with a constant speed prop requires more forethought. Fly a Bonanza as if it were a Skyhawk and trouble will find you in a hurry.
It’s easy to Monday morning quarterback this one, but IMO, the idea of permanently pairing flight crews is fraught with problems. I would consider this practice a contributing factor to this avoidable crash.
Sylvia — can you clarify on avoiding “steep authority gradients”? I never got as far as a commercial license (let alone ATP), but ISTM that green first officers should be paired with solidly experienced captains; otherwise you have the inexperienced leading each other.
As Rudy notes, this reads like a wild-and-woolly pilot who never learned good procedure — and probably was slowly losing the edge that let him survive in Alaska. (cf the saying about no old bold pilots.) Not that the first officer comes off well either — texting while PF sounds like a bad idea at the best of times (because you never know when the times will turn bad), and an even worse idea when the alleged PO is asleep — but a captain doing a less-precise approach just to save a minute of flying time sounds like an invitation to disaster. The point about shuffling crews is especially well-taken; somebody in the rotation might have called this induhvidual on his bad procedures.
Many states have a rule that a certain number of points accumulated for driving offenses causes a license to be suspended; I suppose such a system would be impossible to impose or enforce even if the tower personnel observing such antics were themselves qualified pilots. OTOH, even if the NTSB neglected to gig them for it, the tower personnel didn’t exactly cover themselves with glory either; how busy were they at such a small airport that they didn’t keep up the ATIS or pass on that it was out of date?
Chip,
“Authority gradient” is often used in CRM (crew resources management) courses to describe the authority relationship between the crew members.
A “steep gradient” intends to describe a captain who is the absolute authority in the cockpit and a first officer who just “does as (s)he is told”.
On the other hand, the ideal situation is a gentle gradient, the captain is the person who has the ultimate authority, but makes decisions based on the common knowledge of him- (or her)self, considers and includes the input of the first officer before making decisions.
Usually accompanied by two classic examples. Maybe they have been updated by now, but in my days they were both based on actual flights. Both involved a B727. In the first case, a “steep” gradient, the captain is constantly humiliating the F/O in league with the flight engineer. Comments like “what is the job of a co-pilot?” are answered with: “Sits on his hands, looks out of the cockpit window and says nothing.” It ends with the captain making an approach high and fast. The co-pilot is told to shut up when he comments on that. The whole thing is filmed in a simulator, but the sounds are the actual cockpit voice recordings. The co-pilot is so brow-beaten that he makes not attempt to intervene. The last words were “..I told you so”, followed by the sounds of the crash.
The second example, this time not a “steep” gradient, again was a B 727. Shortly after take-off at night it suffered a nearly total electrical failure. The captain allots tasks, dividing the attention so that the situation can be kept under control. The F/O is flying, the captain is monitoring and goes over the checklists with the F/E. There is nothing in the procedures about the situation they are in. The engineer and the captain, who divides his attention between monitoring the F/O who is using the standby instruments, and the F/E to go over the possibilities, all are doing their work professionally. The F/E then comes with a solution that he thinks may work. The captain considers it and gives his OK. And lo and behold, it worked. The crew regained full control, returned to the airport for a successful landing and Boeing incorporated this into their official procedures to be passed on to all other 727 operators. This was filmed in a simulator and presented to us on successive CRM crouses as a perfect example of an “authority gradient” where the captain did not try to bully his crew, but managed and encouraged them. This lead to an exemplary result. If you prefer, another example of a “steep gradient” can be seen in the White House where anyone who dares to disagree with the president is simply finding him- or herself fired or forced to resign.
I also agree – actually I forgot to include, thanks Chip – that ATC was seriously amiss not updating the ATIS. But under “normal” circumstances this should have led to nothing more serious than a missed approach.
The probem with “points on a driving licence” or, in this case a pilot’s licence, is that the “offences” are not as easily established and the situation in general is more complex. Serious airlines have a very effective in-house system that weeds out the weak links. Records of checks ae kept. For instance, during “command training” I was confronted by the fleet captain with my training record that showed that I had repeated “base training” (a number of approaches and touch-and-goes in the real aircraft, following the simulator training). Fortunately, I could prove that this training was cut short and repeated later, not because I had failed the first session, but because of operational requirements. Another aircraft had mechanical problems and our aircraft was required for a passenger flight.
First off, the outdated ATIS is just one hole in the cheese: the pilot was flying with not a lot of slices between himself and death as it was, doing the approach by the book would have led to a safe go-around and then setting up for the straight-in ILS approach.
I can see why the NTSB has flight data management systems on their “wanted” list: if the company had had such a system, the off-book approaches would have stood out in the data, and the chief pilot could have talked to the crew about it. But it seems they weren’t that concerned about safety anyway.
Reminds me of the lessons some communities are learning in this epidemic: not being concerned about unsafe practices leads to a tough lesson eventually.
Mendel,
You are right, except that the outdated ATIS should not have been a “hole in the cheese” if you mean: a link in a chain of events leading to an accident. The approach plate as copied in this article does not show an ILS approach, but a DME-ARC non-precision approach. But that does not change anything. The QNH or QFE would not have changed dramatically since the issue of the last ATIS. Therefore the MDH or MDA would have been accurately respresented on the altimeter. If the crew had followed the procedure properly it should have led to no more than the nuisance of a missed approach, and perhaps a diversiion, when the crew had reason to believe that they would be able to land. A professionally operating crew must be ready to execute a missed approach, ALWAYS.
It can happen even in good weather conditions, for instance because of a runway incursion.
Before Syposts her new issue:
I had another look at the videos. The Shorts SD 3-30 comes in view in a steep, left wing down angle. Which might confirm my intial suspicion that the captain made a late attempt to turn to finals at too low a speed for the bank angle. Which to me looks as if his final fatal turn may have been to the right; what that means is that the last moments of the aircraft as shown are a desperate attempt to recover from an incipient spin. They would not have had any chance, not from the presumed low altitude.
But this, I hasten to admit, is pure speculation from my side.