Latest Posts – Page 2
The Fatal Flight Instruction: Spiral Dive Technique
A reader contacted me about a fatal crash which killed a pilot and his instructor in November 2021. The reader had some specific questions, which I answered as best I could. However, a few aspects aren’t that clear cut, so I told him I would post it to Fear of Landing and see what other…
Read more… 1 Mar 24
A Brief Word About Icelandic Aviation

Aviation in Iceland started with an airline, not an aircraft. Flugfélag Íslands, the first Icelandic airline, was founded in Reykjavík on the 22nd of March 1919. They did not (yet) have an aeroplane. This was just a few weeks after William Boeing had a C-700 built for himself to explore the exciting new prospect of…
Read more… 23 Feb 24
The Missing Bolts from Alaska Airlines flight 1282

On the 5th of January 2024, Alaska Airlines flight 1282 had just taken off when it lost a door plug, leaving a gaping hole on the left side of row 26. I wrote about the incident that week. The NTSB released a four-minute video of the investigators on the aircraft and I found it interesting…
Read more… 16 Feb 24
Off-roading at Vilnius
On the 3rd of February 2024, an Airbus A320-200, registered in Lithuania as LY-NVL, departed the runway upon landing at Vilnius, Lithuania. This was an Avion Express flight, an operator based in Vilnius that offers seasonal flights to Egypt and performs charter flights for tour operators. Flight NVD8242 was a chartered passenger flight from Milan,…
Read more… 9 Feb 24
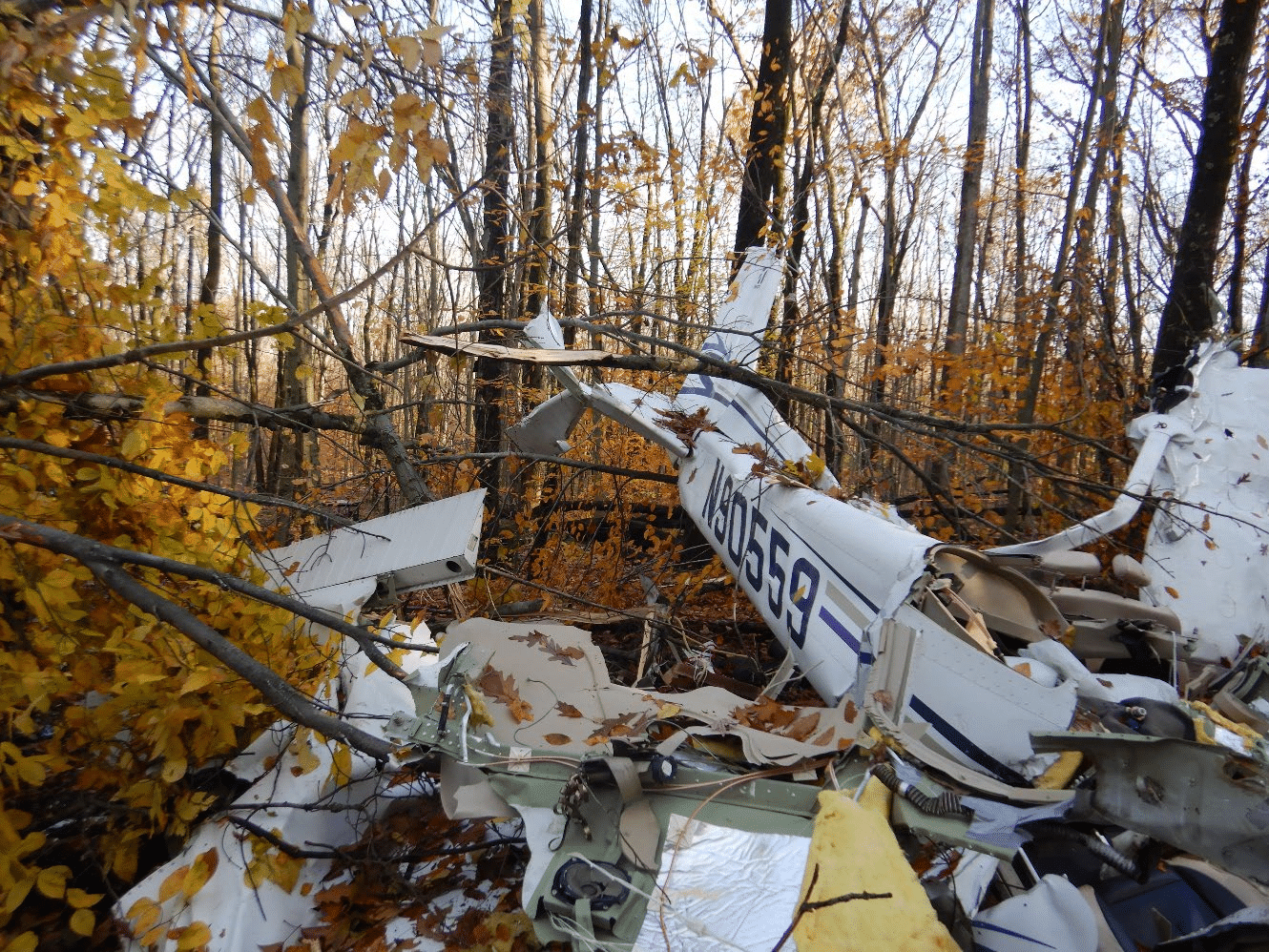
Pilot and ATP student commits suicide using Cessna 172
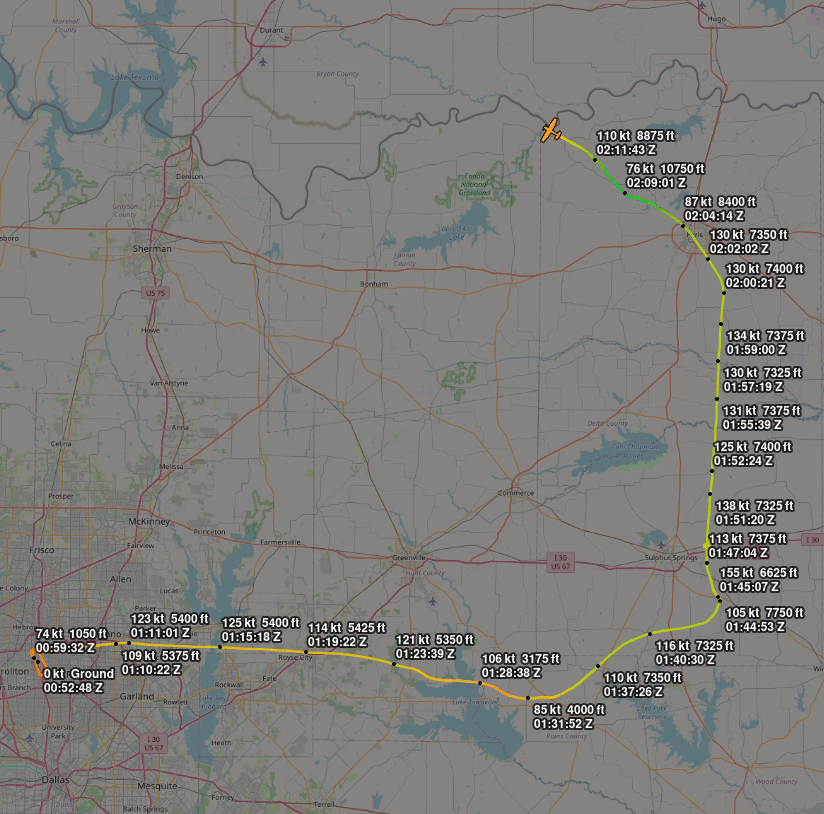
On the 24th of January 2024, a brand new Cessna 172 was stolen from ATP Flight School in Addison, Texas, and deliberately crashed, killing the pilot who was the only occupant. ATP Flight School claims to be the largest commercial pilot flight academy in the US. ATP offers airline-oriented flight training and is said to…
Read more… 2 Feb 24
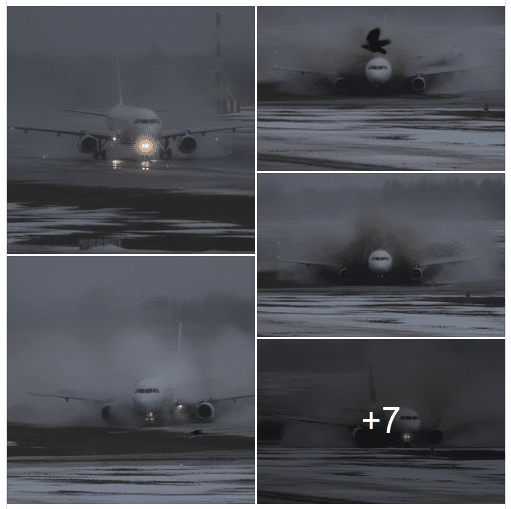
Hard Landing of Turkey’s Vintage Transall C-160

On the 25th of January 2024, videos taken in the city of Kayseri showed a Turkish Air Force C-160 Transall aircraft flying dangerously low towards Kayseri Erkilet Airport in Turkey. Ekibin eline sağlık, şehir içerisinde bir kazaya sebebiyet vermemişler. pic.twitter.com/JfOvk5HbsF — TangoTangoLima (@Ttltlg) January 25, 2024 Kayseri Erkilet Airport is both a military air base…
Read more… 26 Jan 24
Accident Reports
 Madness on the Runway at Manchester
Madness on the Runway at Manchester
The Manchester Airport Group Plc owns and operates three airports: Manchester, London Stansted and East Midlands. Manchester Airport is the third busiest airport in Britain. Their website says Manchester Airport…
 Mid-air Collision of Wingsuit Flyer and Pilatus PC-6
Mid-air Collision of Wingsuit Flyer and Pilatus PC-6
On the 27th of July 2018, an experienced pilot departed with ten parachutists on board for a routine drop mission. It was the pilot’s fourth flight of the day in…
Demystifying
 Training an AI Copilot To Spot Gliders
Training an AI Copilot To Spot Gliders
My friend Maria at Daedalean wrote this article about how they are using AI to help pilots detect gliders. I thought it was fascinating and Daedalean gave me permission to…
 Descending into Illusion: The Black Hole Effect
Descending into Illusion: The Black Hole Effect
With no moon or city lights to guide you, the runway lights up ahead should be a beacon of safety. However, it might be a trap known as the black…
History
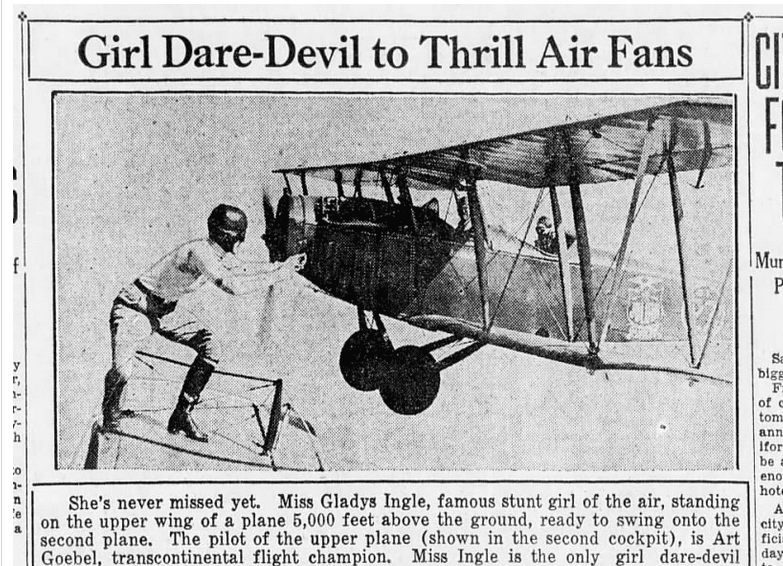 Gladys Ingle Inflight Wheel Change: Emergency Action or Stunt?
Gladys Ingle Inflight Wheel Change: Emergency Action or Stunt?
This video of a mid-air wheel exchange goes viral once a year or so, but I never get tired of watching it. Last week, it showed up on Reddit and…
 The Disappearance of the Hawaii Clipper May Not Be as Mysterious as Was Thought
The Disappearance of the Hawaii Clipper May Not Be as Mysterious as Was Thought
This week, we have a guest post by J.B. Rivard who wrote an article for the American Aviation Historical Society (AAHS) and used one of my articles as a reference.…
Fun Stuff
 A Few Good Stories
A Few Good Stories
I’m in Dresden at the moment and I’m afraid I haven’t had a free moment to write you a new article. Luckily, lots of other people are on the internet…
 Flying Fails and Airshow Considerations
Flying Fails and Airshow Considerations
Long-term readings of Fear of Landing know that my favourite aerobatics show of all time is Kyle Franklin’s Ben Whabnoski Comedy act. Just in case some of you haven’t seen…